Injection Technique
When considering treatment with botulinum it is important to remember the anatomical structures DO want to relax; corrugators, orbicularis and the structures we DO NOT want to effect; frontalis, orbital structures such as the lacrimal gland or elevators.
The orbicularis, a the most superficial, naturally acts as a protective barrier to the muscles we want to avoid affecting with toxin. We can utilise such natural barriers when injecting to help us safety net the structure we do not want to incorporate into treatments, while still achieving the desired result.
As I’m sure you have already been practising, the recommended distance laterally for injecting toxin to treat the orbicularis is 1 -1.5cm around the eye, from the orbital rim, to treat the crow’s feet area. Safety consideration doesn’t just start and stop here, as the depth of the needle’s penetration is equally as important.
The consideration of needle depth is highly applicable when treating the corrugator complex at the orbit superiorly.
To unintendedly prohibit the action of the nerves and tissues under the orbicularis muscle, the toxin must be placed underneath it. However, in order to effectively treat the corrugators you will need to inject under the orbicularis oculi. Therefore, this is likely the most probable cause of lid ptosis from botulinum injections.
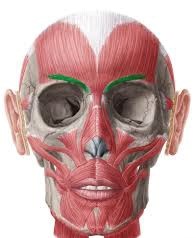
ANATOMY OF CORRUGATOR
- Starts deep at level of bone
- Moves laterally from medial superciliary arch
- As it does it becomes more and more superficial in the tissues
- Inserts at level of orbicularis oculi into the skin
- Lateral to mid pupillary line
We can vary technique of injection in 3 main ways; depth, dose, angle
Where the corrugator is deep a higher dose of toxin will be safe, around 4 units. Parallel positioning is best in more superficial parts of the muscle so to avoid the orbital rim or frontalis. The dose can then be adjusted accordingly as you reach the muscle laterally to the mid pupil. Angle of insertion, again, should avoid the orbital rim; 30 degrees lateral to 45 degrees medial to help reach the right depth.

