How blindness occurs as a result of treatment location
The Glabella
By far one of the highest risk areas when injecting dermal filler, given this area can usually and effectively be treated with botulinum toxin, we do have to assess and ask ourselves – does the benefit of treatment outweigh the risk. It is of my opinion and gold standard practice those general practitioners and injectors should not be injecting filler into the area and is regarded as specialist, meaning facial plastic surgeons and other such clinicians should be competent in their skill to administer this treatment. Anatomically the Glabella is almost always with extreme proximity of the supratrochlear artery, being just a few millimetres between the hypodermis, muscle and lower dermis where the artery resides. The supratrochlear artery branches off to supply the ophthalmic artery. Injury to such during a procedure would have catastrophic detrimental effect to all areas in the orbit. As you can now appreciate it is an area to be avoided at all costs when injecting filler unless an extremely experienced and highly skilled medical/surgical aesthetician.
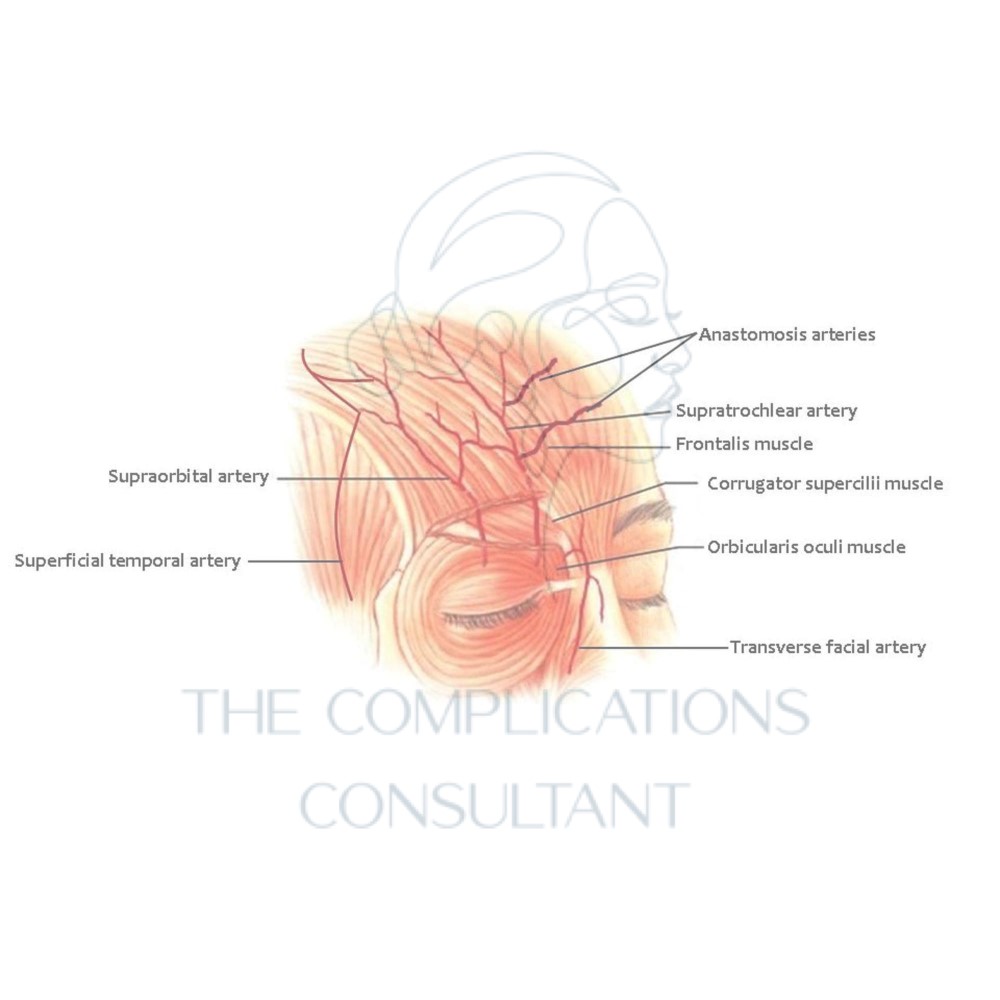
The Forehead
Again, the supratrochlear artery and its occlusion is a risk factor at play when considering treatment of the forehead, in addition to this you need to also consider the positioning of the supraorbital artery, both of which branch off the ophthalmic artery. Another connecting artery in relation to the previous is the superficial temporal, therefore low viscosity filler could even pass through the temple and into the ocular circulation.
Not surprisingly the dorsal nasal artery is a main player in the risk of causing occlusion when injecting into this area, again the supratrochlear is also at risk. Aspirating the needle for at least 10 seconds is always advised when injecting the saddle of the nose and the bridge alike. Superior vessels of the nose are very closely connected with blood supply of the orbit. Asian countries in particular tend to inject high volumes of filler into these high-risk areas, meaning prevalence of occlusions happening are much higher. The use of cannula and needle can both be responsible for injury.
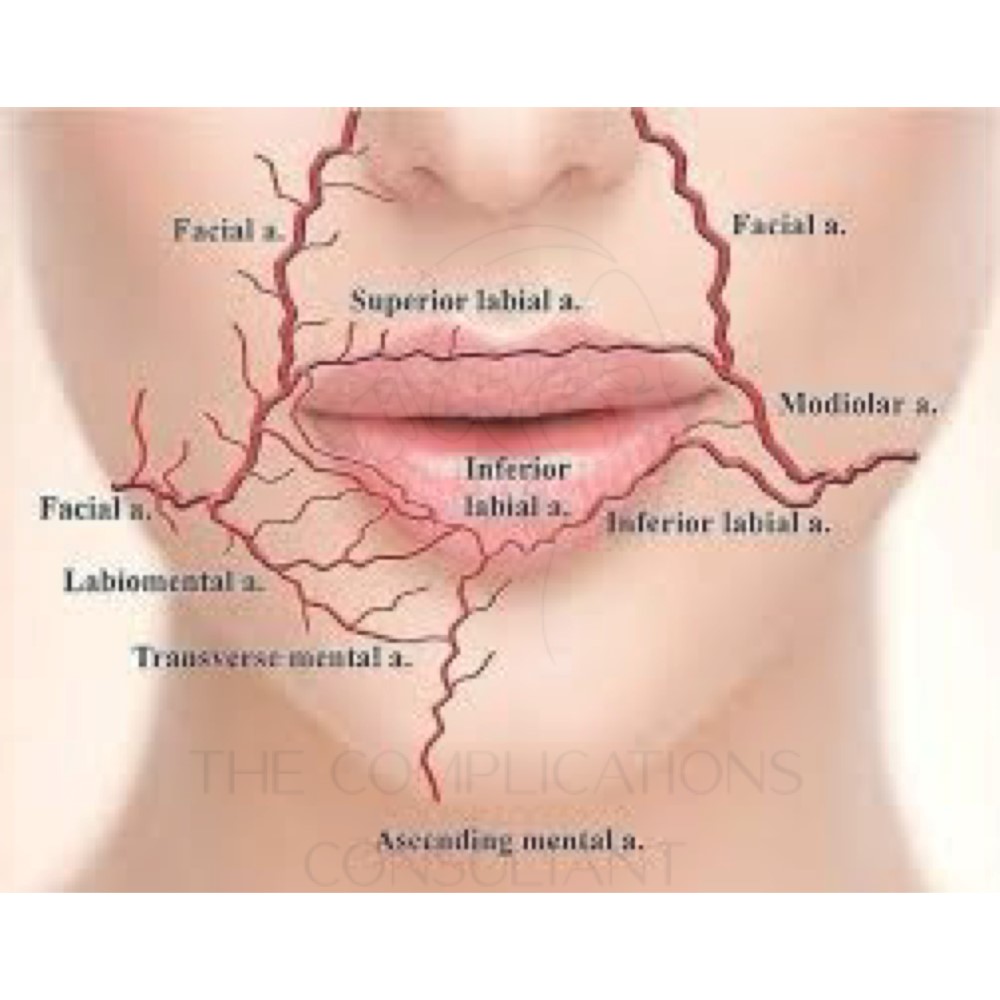
The Nasolabial Fold
Generally speaking, there is usually only about 5mm space between the facial artery and where the nasolabial fold sits. It sits under the dermis in the fatty layer and has direct access to the supratrochlear artery via the angular artery. The emboli or causative blockage can travel along this pathway to cause visual disturbance. The riskiest way to place filler here is in a fanning technique at the alar base, cannula and periosteal techniques should be favoured in the interest of patient safety.
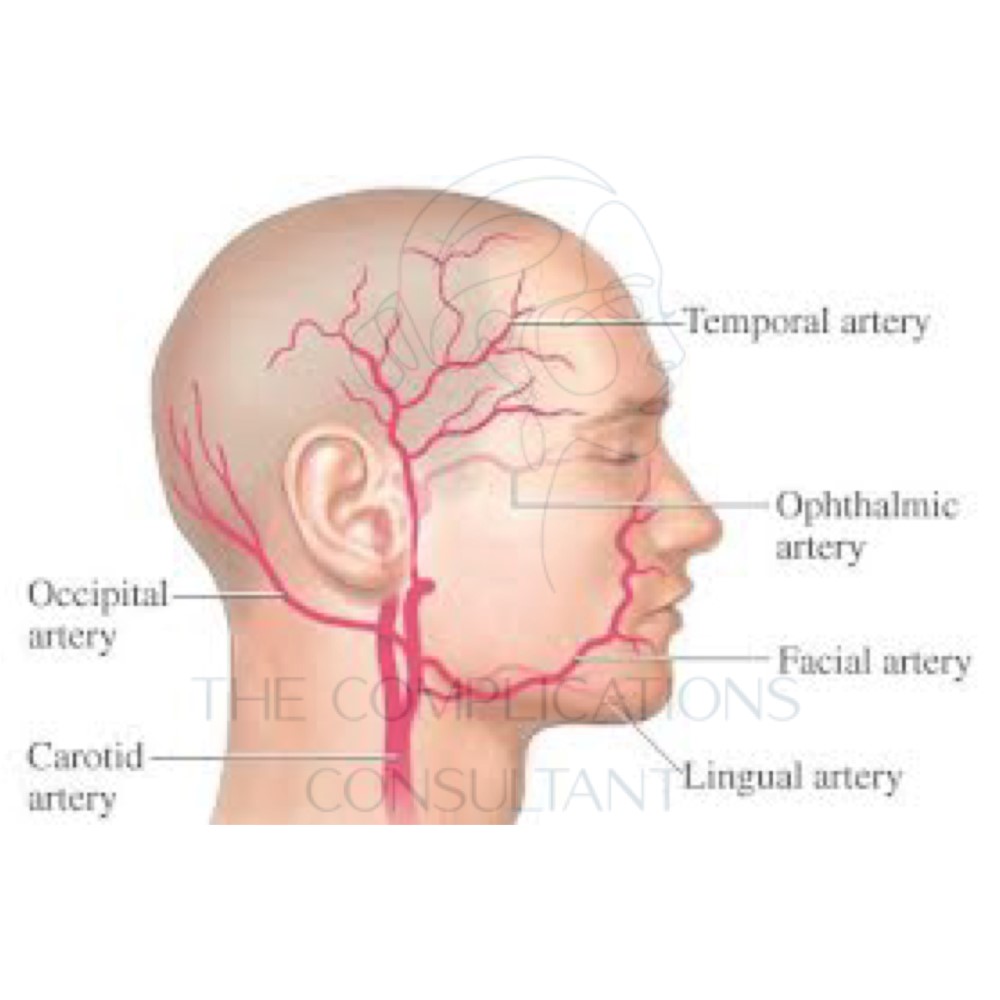
The Temple
Several possibilities arise from the temporal area when considering dermal filler and arterial blood supply complications. It has been evidenced that fluid could possibly pass from superficial temporal artery into the ophthalmic system by diffusion along the forehead, in cadaver studies. Thus theoretically also effecting supratrochlear, supraorbital, and lacrimal arteries.
Periocular Injections
The cause for several cases of blindness
LATERAL CANTHAL LINES AND TEAR TROUGH
- In Asian countries such as north Korea and China they will happily place filler into the eyelid
- It is believed the bulge gives rise to a more happy and smiling face
- This is very dangerous due to the anatomical structures of course
- But notwithstanding the potential possibility for low viscosity product to flood vessels of the ophthalmic vessels.
THE EYELID
- Venus drainage of the eye connects to the canvernous sinus
- This can be impacted if the vorticose veins are blocked
- Occluding the inferior ophthalmic or inferior palpebral vein will be a reason for this
The Tear Trough
- Damage likely to affect the angular artery
- Angular artery runs lateral to the nose and medial to tear trough
- In a study 32% of cases had anatomical derivations of the standard typical positioning of the angular artery, making the procedure riskier as it was closer to the tear trough area.
- In these cases, the artery lays in the cheek more vertically instead of laterally
- What this means for risk, is it is at higher risk if occluded to follow a pathway to the orbicularis oculi near the retaining ligament sits, another risk area for tear trough filler.

The Cheek
- Low risk area
- Only one recorded case and this was not with the use of dermal filler but of fat
- Most likely cause would be medial cheek injection affecting angular artery
- This could be direct or by an anastomosis of transverse facial artery
Let’s now consider how the different materials may affect the chances of blindness from dermal filler.
Main contenders are of course dermal fillers of hyaluronic acid but another would be the injection of fat into an area. Fat is used in much higher volumes than HA dermal filler. This will obviously hold higher risk as a result, the biggest review showing a 61% chance of recovery of sight when using HA dermal filler as opposed to 21% when using fat. This went on the review that the most common causes of strike and then death were caused by injecting fat. There has been one reported incidence in the UK in 2012, of stroke by injection of Sculptra into the temple, this product is made up of poly L lactic acid

